

Abstract
Background. The availability of multiple tyrosine kinase inhibitors (TKIs) and precise molecular monitoring has dramatically changed the prognosis in CML patients. With proper medical management, the planning of a pregnancy in both male (M) and female (F) patients is now possible. Towards this goal, the GIMEMA CML working party initiated a retrospective and prospective study to describe all male conceptions/female pregnancy outcomes in the CML Italian population from January 2013.
Aims. The specific aims of this study were to analyze conceptions and pregnancies in male and female patients with regard to 3 general issues: 1) Illness issues, including CML treatment prior to conception/during/after pregnancy, transcript kinetics, the recovery of a lost response after therapy cessation, and the effects of treatment modifications (e.g., resistance, switching); 2) Conception/pregnancy issues, including planned, unplanned, spontaneous and medically assisted pregnancies (MAP), spontaneous/elective abortions, pregnancy progression, delivery, and breast feeding; and , 3) Post-natal health issues from birth to walking including speaking and academic performance.
Patients and methods. Patients included in the study had to meet the following criteria A) Age >18 yrs; B) Confirmed CML diagnosis; C) Conception or pregnancy; D) TKI treatment before, during and/or after pregnancy; and E) Signed, IRB-approved written informed consent form. Of the 143 enrollees, data were obtained from 135 patients (83M and 52F). A total number of 166 cases were analyzable. Male conceptions were 106, and female pregnancies 60.
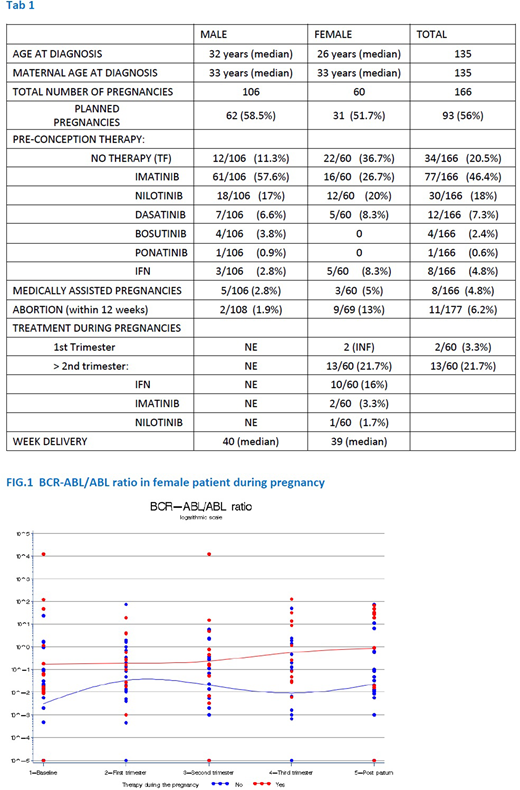
Results 1) At time of conception 34 patients had no treatment (TF), 8 received interferon-a (IFN), and the remaining were treated with a TKI (Table 1). Considering only female patients, all stopped TKI treatment when pregnancy was discovered at 3-6 weeks (w). After placental maturation (>20w) 13 patients were treated with IFN (10), 2 with Imatinib, and 1 with Nilotinib (N). In this latter patient N concentration was tested in maternal plasma and cord blood at delivery and showed no transfer to the baby. Kinetics of rise was calculated in a subgroup of 17 patients. Doubling time [DT = duration x log(2) /log (final ratio)-log (initial ratio)] exhibits a bimodal trend, very short for some patients (5.8 days mean, range 4.5-8.2) and much longer for others (182 days mean, range 59.2-328.4), This result does not correlate with molecular status pre TF. Furthermore 76.5% of patients will not lose Major Molecular Response during pregnancy, while in TF, that is more than expected when compared to non pregnant controls (TFR). No cases of CML progression or resistance to re-treatment were observed. CML transcript ratios during pregnancy are shown in Fig.1.
2) The majority of pregnancies were planned. MAPs were reported in 5M and 3F. Two spontaneous conceptions occurred in 2M after allogeneic transplant. Eleven abortions before 12 w (2 M ,induced; 9F, 5 induced) were reported (not included in the 166 cases). Pregnancies in all cases progressed normally. In F there were 2 pre-eclampsia, 2 oligohydramnios, 1 abruption placenta. In 8M and 8 F babies were born pre term and 1M and 2F were small at birth with no further consequences. Forty-two F (70%) delivered spontaneously. Babies were born at a mean 40 w (34-44) in M, 39 w (33-42) in F. Breast feeding information was collected for 45F of which18 (29%) breast feed for at least one month (range 1-28 mo).
3) Post-natal information showed normal child development and growth. One respiratory arrest was noted at birth with rapid recovery and 1 macrocephaly was described with no further consequences. Of the 56 children >3 yrs old attending school (44M,12F), 2M presented with language problems and in one case autism was diagnosed. Other reported outcomes include 1 child diagnosed as having rheumatoid arthritis at 2 yr (F), and 1 diagnosed with celiac disease (M).
Conclusions TKI therapy has allowed CML patients to pursue a normal life including planning/managing a family. Males do not need to stop therapy to conceive due to the therapy's non-genotoxic nature, in contrast to females who must cease therapy due to the teratogenic nature of TKIs. Kinetics of regrowth of the CML residual disease during pregnancy in female patients is different than in TFR patients. To our knowledge this is the largest multicentric study regarding CML and reproduction. Results and practical management will be presented.
Abruzzese:Novartis: Research Funding; Pfizer: Consultancy; Ariad: Consultancy; BMS: Consultancy. Castagnetti:Incyte: Consultancy, Honoraria; Bristol Myers Squibb: Consultancy, Honoraria; Novartis: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria. Gambacorti-Passerini:Pfizer: Consultancy, Honoraria, Research Funding; BMS: Consultancy. Rambaldi:Pfizer: Consultancy; Novartis: Consultancy; Italfarmaco: Consultancy; Omeros: Consultancy; Roche: Consultancy; Celgene: Consultancy; Amgen Inc.: Consultancy. Gaidano:Roche: Consultancy, Honoraria; Morphosys: Honoraria; AbbVie: Consultancy, Honoraria; Gilead: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Amgen: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal